Poststroke Brain Herniation Syndrome
Sub-falcine and an impending transtentorial herniation by Pavly G.
Keywords:
Neurosurgery - Neurocritical care - Stroke Syndromes - Case Report - Cushing’s Reflex - Sub-falcine Herniation - Transtentorial Herniation - Decompressive Hemicraniectomy
Introduction:
Stroke syndromes are one of devastating issues that could lead to a subsequent critical increase in intracranial pressures especially in the case of Massive Stroke Syndromes (e.g., Massive P. Cerebral a. Stroke).
To better study the sequence of actions that could lead to the subsequent increase in the intracranial pressures and eventually brain herniation through brain meninges or foramen magnum; it is better to study what really happens when an imminent stroke takes place in an ischemic penumbra.
Biophysics in a closed cavity:
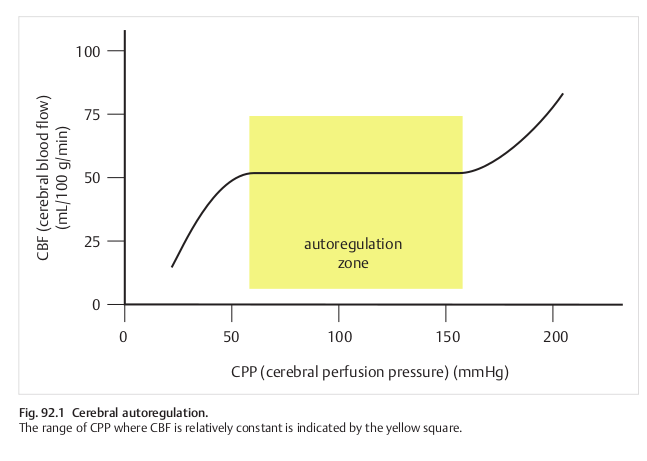
The intracranial pressure (ICP) is one of the most essential physiologic parameters in determining cerebral perfussion pressure (CPP), and subsequently the cerebral blood flow (CBF).
It’s noted that; as the ICP increases linearly; the CPP decreases, and as a result, the CBF decreases; this could be counter-parted by increasing the mean-arterial blood pressure (MAP) until a specific offset is reached, in which the cerebral auto-regulation gets compromised (i.e., De-compensation of the physiological autoregulatory reflexes).
Increasing the mean-arterial blood pressure entails either increasing the cardiac output (CO) components or the Capillary Systemic Vascular Resistance (SVR) or both.
Case Presentation:
A 62-year-old male, known CKD patient, presented with disturbed conscious level; evaluated as GCS of 13/15 with E(4)-V(4)-M(6), after receiving 1 unit of packed RBCs to correct his anemia of (HB=7.6 mg/dl), most likely attributed to a early blood transfusion reaction (within 24 hours); manifested as fever and disturbed conscious levels.
The patient was transferred to the ICU as result of possibility of developing transfusion-associated sepsis. Hours later at the same day; the patient developed right hemiplegia with dysphasia. After which, it’s not well-documented whether the patient has entered a state of impaired consciousness within hours from the massive stroke or at the same time of the stroke.
Remark (01):
It’s essential to know this piece of information; as it could determine whether the patient has developed a brain herniation syndrome right after the massive stroke or the patient has developed a brainstem infarction coincidentally simultaneously with the massive stroke at the level of the tegmentum involving the Ascending Reticular Activation System (ARAS).
Remark (02):
In any ways, in case the information is distorted, one could rely without hesitation on the objective data; typically the Angiogram Studies; Cerebrovascular CT Angiogram and Perfussion CT or MRI with MR-DWI and MRA/MRV; either of which are of great use here to attain the viability of the brainstem structures before deciding whether this patient has entered that state of imparied consciousness as a result of the mass effect and the increased intracranial pressure requiring an emergent Decompressive Hemicraniectomy, or another acute ischemic stroke event is simultaneously the reason for this state of impaired consciousness.
Remark (03):
Uncontrolled hyperglycemic crises are almost always an attributable component to developing acute ischemic stroke syndromes of thrombotic origins; the pathophysiology entails; in part due to the high serum lactate and anaerobic cellular respiration rate that activates the anti-insulin systems (i.e., Metabolic Pituitary-Hepatic-Adrenal Axis) leading to further hyperglycemia, hypertension, acute dyslipidemia, vascular endothelial injury which in turn activates the coagulation cascade and a severe type I inflammatory reaction leading to thrombosis of the vascular lining.
Therefore, the following are diagnostic studies that should be attained as fast as possible:
-
Obtain two large bore IV Cannula Access to the antebrachial veins (e.g., Green 18G) whenever possible before bridging to CVC.
-
Continously monitor the blood pressure and arterial oxygen saturation.
-
If anaphylactic shock is suspected; activate the code and start resuscitation immediately.
-
Obtain a Bedside Glucose Measurement (BGM).
-
Obtain an ABG with Serum Lactate to profile the patient metabolic panel.
-
Start slow IVI of 500ml Saline until labs are available.
-
Obtain at least a chest x-ray to rule-out Transfusion-related acute lung injury (TRALI) that resembles the same clinical manifestation and management as ARDS.
-
Multislice NECT of the brain (Axial, Coronal, Oblique, and Sagittal).
-
Cerebrovascular CT Angiogram with reconstruction format.
-
An Echocardiogram looking for mural and atrial thrombosis, structural heart abnormalities (e.g., atrial myoxomas or atrial septal aneurysms), and hypo/dyskinesia.
-
Continous EKG monitoring for AF, electrical signals from accessory pathways, other and Atrial Arrhythmias signifying a suspected source of thromboembolism and Cerebral Hypoperfusion syndromes (Adams-Stokes Attacks), respectively.
-
Full blood count (FBC), and Coagulation Studies (Coagulation Profile and D-dimer).
Late Clinical Findings (2nd day):
Late clinical findings are highly suggestive of either an ensuing brainstem stroke has took place right after the MCA/ACA stroke or simultaneously, or disturbed consciousness as a result of a subfalcine herniation syndrome.
Neurological examination revealed a Glasgow-coma scale (GCS) of 5/15; specifically E(1)-V(1)-M(3), in which the motor component shows an abnormal flexion posture (i.e. Decortication) reflecting a probable lesion in the corticobulbar tracts and/or the cerebral cortex.
Brainstem assessment revealed bilateral non-reactive pupillary light reflex (PLR) component, and impaired vestibulo-ocular reflex (VOR) component signifying brainstem involvement with the diffuse modulatory systems involvement.
Quadriplegia was noted with areflexia in all limbs, and positive planter extensor response on the right side.
GCS (Glasgow Coma Scale)
| Component | Description | Score |
|---|---|---|
Eye |
Spontaneous = 4 |
1 |
Verbal |
Orientated = 5 |
1 |
Motor |
Obeys commands = 6 |
3 |
Pupils Light Reactivity |
Both non-reactive = 2.0 |
2 |
GCS = (5)/15, E(1)V(1)M(3). GCS-P = (3)/15.